70year old male with involuntary movements in left upper and lower limb
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case presentation:
A 70year old male patient who is a farmer by occupation came with chief complaints of involuntary movements in the left upper and lower limb from two days.
HOPI:
Patient was apparently asymptomatic two days back then developed involuntary movements in left upper and lower limb.the movements were seen for every 5 to 10mins .
H/o frothing, up rolling of eyes and drowsiness present
H/o post ictal confusion present
H/o generalised pitting type of edema from one week.
No H/o loss of consciousness ,vomitings,headache,trauma
No h/o difficulty of breathing and fever.
PAST HISTORY:
K/C/O CVA left sided hemiplegia two years back (april2018) - middle cerebral infarct seen
K/C/O ? Acute motor axonal neuropathy variant of GBS , LMN type of momoparesis of left upper limb 2years back.
No h/o HTN DM TB asthma cardiac abnormalities
H/o surgery ( unknown - reports are not available ) for acid ingestion 6years back.
H/o similar episodes of involuntary movements in left upper and lower limb 20 and 45days back resolved spontaneously.
PERSONAL HISTORY:
normal appetite
Adequate sleep
Normal bowel and bladder movements
Addictions - smoker from 45yrs
Alcoholic from 45yrs
GENERAL EXAMINATION
Patient is conscious coherent and irritable
Moderately built and moderately nourished
Pallor present
No icterus clubbing cyanosis lymphadenopathy
Generalised pitting type of edema present
SYSTEMIC EXAMINATION
CNS : not oriented
Rt Lt
Bulk N N
Tone UL N Increased
LL N Increased
Power UL N Not elicitable
LL 4 3
Reflexes biceps - 1+
Triceps - 1+
Supinator - -
Knee - -
Ankle - -
Plantar - Up going
CVS S1 S2 heard no murmurs
GIT no organomegaly non tender
RS BAE Present coarse crepts present
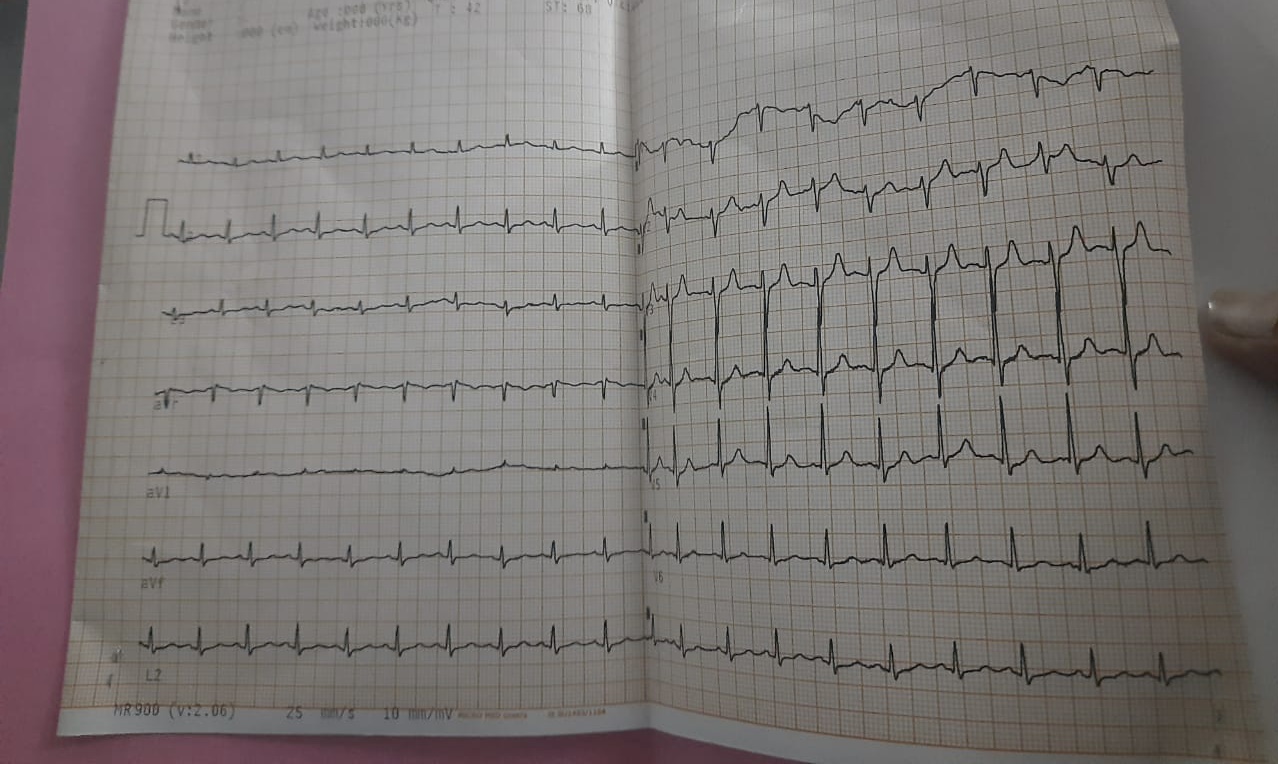
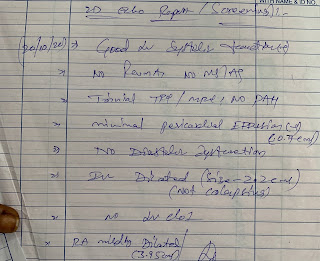
INVESTIGATIONS:


















Comments
Post a Comment