66 year old patient with generalised weakness.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case presentation:
66yr old male patient who is watchman by occupation and resident of suryapet came to general medicine opd with complaints of generalised weakness from one week and involuntary movements of right upper and lower limbs from 3days.
HOPI:
Patient was apparently asymptomatic one week back then developed generalised weakness which is predominant in lower limbs associated with difficulty in walking, standing with support,difficulty in rolling on the bed from side to side.
Complaints of involuntary movements in right upper and lower limb lasting for 2mins multiple (5 to 6) episodes per day from 6days ,not associated with loss of consciousness,up rolling of eyes , frothing, bowel and bladder abnormalities, not progressing to left side.
No h/o headache, trauma.
PAST HISTORY :
K/C/O of CVA with left hemiplegia 4yrs back with left LMN type facial palsy discontinued antiplatelet 3yrs back .
K/C/O DM -2 from 2years on OHA discontinued medication from two months
K/C/O HTN from one year discontinued medication from two months
Mute since birth.
PERSONAL HISTORY:
Mixed diet
Adequate sleep
Normal bowel and bladder movements
Normal appetite
Occasional alcoholic non smoker
GENERAL EXAMINATION:
No pallor, icterus,cyanosis,lymphadenopathy,pedal edema.
Dry scaly pruritic patches seen on various regions of the body
Dermatology referral was taken in view of these patches and diagnosed as Tinea corporis et cruris
Zoderm -e was advised for local application.


VITALS:
Afebrile
BP:170/90mm hg
Pulse rate : 58bpm
GRBS : 474mg / dl
SYSTEMIC EXAMINATION:
CNS
higher mental functions could not be assessed
Tone : UL LL
Right Normal Normal
Left. Normal. Normal
Power: Right. Left
Handgrip. 60% 100%
UL proximal 4-/5 4-/5
Distal 5/5 5/5
LL proximal 4+/5 4+/5
Distal 4+/5 4+/5
Reflexes :
Right - Brachial , triceps, supinator absent
Knee 2+ , ankle +, plantar exaggerated
Left - Brachial , triceps, supinator absent
Knee 2+ , ankle +,plantar exaggerated
RS:
Bilateral air entry present
No wheeze no crepetations
GIT :
Soft , non tender ,no organomegaly.
CVS :
S1 S2 heard no murmurs
INVESTIGATIONS:
27/10/2020
Urine for ketone bodies positive
RFT
Urea 40
Creat 0.9
Uric acid 2.8
Ca 10
Phosphate 3.6
Na 137 K 3.9 Cl 102
CUE
Albumin | trace
Sugar - ++++
Pus cells - 5 to 6
Epithelial cells - 2 to 3
RBC
27/10/20
ABG 3AM
Ph - 7.379
Pco2 100
Po2 100
K -2.4 Ca - 0.35 Cl- 91 Na - 134
ABG 6AM
PH 7.329
PCO2 30.1
PO2 101
HCO3 17.2
28/10/20
LIPID PROFILE
Total cholesterol 102
Vldl 18.5 TG 94 Hdl 30 ldl 63
FBS - 119
Urine for KB positive
CBP
Hb 12
Tlc 13000
Plt 1.94
SERUM ELECTROLYTES
Na 143
K 4.1
Cl 105
ABG 1pm
PH 7.41
Pco2 28.9
Po2 103
Hco3 18.1
St hco3 19.9
CHEST XRAY

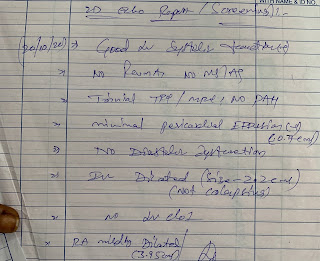
2D ECHO






Comments
Post a Comment